Recently, this has become a trend among politicians and organizations: draw a line in the sand (if possible, draw the line in a red color), with an accompanying threat – if you cross this line we (or I) will do so-and-so. The intention is to frighten the object of our scorn away from crossing the line.
A recent example came in context of the Syrian civil war when President Obama remarked on the threat issued by Syrian president Assad that he would use chemical weapons on his own people. As reported in the Washington Post, President Obama said:
“We have been very clear to the Assad regime, but also to other players on the ground, that a red line for us is we start seeing a whole bunch of chemical weapons moving around or being utilized. That would change my calculus. That would change my equation.”
Well, the general understanding was that if the Assad regime crossed the line and used chemical weapons, the American government would respond with active participation in the fight against the regime. Shortly after the statement was made, it was proven that the Assad government did cross the line, and the world was staring at President Obama to respond.
The response was not in the form of actual military involvement, but in the form of an agreement with the Russian government and with the Assad government for a controlled removal and eventual disposal of chemical weapons from Syria. Most of the world saw it as a sign of American unwillingness to get directly involved with the ramifications about the consequences of crossing other “red lines.”
Back to climate change – In a recent segment (the 4th segment that was aired on May 4th) of the Showtime program “Years of Living Dangerously” (see the April 22, 2014 blog), reporter Lesley Stahl asked an American scientist who took part in writing the recently published IPCC (Intergovernmental Panel on Climate Change) Fifth Assessment Report, what, in her opinion, was the most important part of the report. (I will report on my general reaction to the Showtime program once it completes its nine segments.) The answer was that IPCC was “drawing a line” on the question of how much unburnable carbon needs to be left in the ground in order to limit the damage from climate change to an “acceptable” level of 20C (close to 40F).
This particular “red line” was selected based on the following quote from the Summary for Policy Makers of Working Group I of the Fifth IPCC Report (WGI of AR5). (It took me some time to locate the quotation out of the combined report which contains more than 3000 pages.)
E.8 Climate Stabilization, Climate Change Commitment and Irreversibility
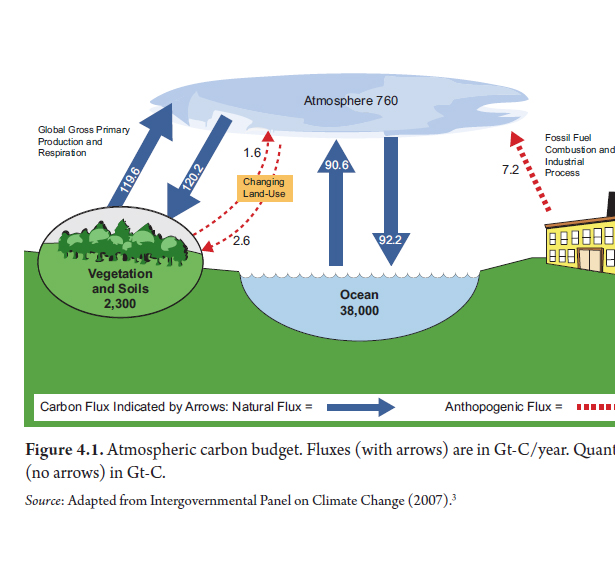
Cumulative emissions of CO2largely determine global mean surface warming by the late 21st century and beyond (see Figure SPM.10). Most aspects of climate change will persist for many centuries even if emissions of CO2 are stopped. This represents a substantial multi-century climate change commitment created by past, present and future emissions of CO2. {12.5}
• Cumulative total emissions of CO2 and global mean surface temperature response are approximately linearly related (see Figure SPM.10). Any given level of warming is associated with a range of cumulative CO2 emissions21, and therefore, e.g., higher emissions in earlier decades imply lower emissions later. {12.5}
• Limiting the warming caused by anthropogenic CO2 emissions alone with a probability of >33%, >50%, and >66% to less than 2°C since the period 1861–188022, will require cumulative CO2 emissions from all anthropogenic sources to stay between 0 and about 1570 GtC (5760 GtCO2), 0 and about 1210 GtC (4440 GtCO2), and 0 and about 1000 GtC (3670 GtCO2) since that period, respectively23. These upper amounts are reduced to about 900 GtC (3300 GtCO2), 820 GtC (3010 GtCO2), and 790 GtC (2900 GtCO2), respectively, when accounting for non-CO2 forcings as in RCP2.6. An amount of 515 [445 to 585] GtC (1890 [1630 to 2150] GtCO2), was already emitted by 2011. {12.5}
These limits require that we leave about 70% of the fossil resources in the ground and never use them as fuels. In the “business as usual” scenario, it is estimated that this “red line” will be reached around 2040. The implications of this “unburnable carbon” were explored before (see July 17, 2013 blog) and there is no question that the issue of energy transition to non-carbon energy sources is the central message that IPCC is trying to convey in its reports. The question is what will happen if, by 2040, we will fall short; should we give up and say collectively to ourselves that we cannot make it and continue in our merry ways?
In the September 3, 2012 blog, I described one of the three shades of deniers in the following way:
(2) The fatalists. This group fully agrees with both the science and its predicted impact, but believes that since the task of preventing it (global warming) is so enormous as to be practically undoable, they might as well enjoy life for as long as it lasts. Unfortunately, many in this group are good scientists.
Crossing the “red line” on the 20C clearly satisfies such an attitude. The show “Years of Living Dangerously” is obviously not the only voice that puts the line in the sand at this temperature. Many environmental organizations are also drawing such lines, since it appears to be an attractive and understandable message that helps mobilize public support. See this, for example.
Probably the most famous organization to do this is 350.org. This is an international organization with wide support and access to funding and media. They describe themselves in the following way:
350.org is building a global climate movement. Our online campaigns, grassroots organizing, and mass public actions are coordinated by a global network active in over 188 countries.
The number 350 means climate safety: to preserve a livable planet, scientists tell us we must reduce the amount of CO2 in the atmosphere from its current level of 400 parts per million to below 350 ppm.
350 is a smaller number than 400 ppm, our present global level of atmospheric carbon dioxide. To achieve this level, we not only have only to stop, cold-turkey, emitting any new carbon dioxide, but we also have to start an effort to remove some of atmospheric carbon dioxide by using geoengineering techniques that were described in the previous blog.
Politically, such an effort seems beyond reach and the alternative might be to resort to doing nothing. Therefore, a more productive long-term alternative seems to be an emphasis on the process of energy transition and the adaptive tools that need to be employed in the transition to more sustainable energy use.